


The Health Benefits of Easter Chocolate
It’s the month of Easter. What better way to celebrate than to talk about chocolate’s warm, milky goodness? Everyone has a favourite, but if you want our opinion (or read up on the latest health research, which we do a lot – something of an occupational hazard for osteopaths) the darker the chocolate the better it is for you. But that doesn’t mean we recommend you demand dark chocolate and nothing but dark chocolate from the Easter Bunny. Why? Read on to find out.
It’s the month of Easter. What better way to celebrate than to talk about chocolate’s warm, milky goodness? Everyone has a favourite, but if you want our opinion (or read up on the latest health research, which we do a lot – something of an occupational hazard for osteopaths) the darker the chocolate the better it is for you. But that doesn’t mean we recommend you demand dark chocolate and nothing but dark chocolate from the Easter Bunny. Why? Read on to find out.
Dark chocolate is generally considered better for you than other varieties because it contains a higher percentage of cocoa solids. Cocoa solids contain antioxidants called flavonoids, which research has associated with several health benefits, including:
• Improved heart health: Flavonoids can help lower blood pressure, improve blood flow, and reduce the risk of heart disease.
• Better brain function: Studies suggest that the flavonoids in dark chocolate can improve cognitive function and reduce the risk of neurodegenerative diseases like Alzheimer's.
• Reduced inflammation: Antioxidants help reduce inflammation in the body, which has been linked to several chronic health conditions.
By its nature, dark chocolate contains less sugar than the hyper-sweet stuff. Plus, we know sugar can increase inflammation in the body, be addictive, trigger bizarre insulin reactions, and contains nutritionally useless calories (oh, and it’s a nightmare for your oral hygiene too). But it’s important to remember that it still contains some sugar and fat so you should enjoy it in moderation! But what if you don’t enjoy it? That’s OK – you can get flavonoids from tea, fruit and vegetables. It’s not an essential part of your diet – after all if your ancestry is European, Australasian, African, Asian, or North American (anywhere but South America) your ancestors survived without it for tens of thousands of years!
So, I Should ONLY Eat Dark Chocolate, Right?
But with all those health benefits why would we suggest you shouldn’t celebrate Easter with a dark chocolate frenzy? As osteopaths, psychology isn’t our main thing, but we do know our patients. We know that the exercises we prescribe need to be more than “good for you” they need to be achievable for where you are right now - and maybe even a little bit fun. With that in mind we suggest that the healthiest chocolate is one you enjoy: one you can take a bite or two of and feel satisfied. If you don’t like dark chocolate you’ll eat it, and then probably eat some more because you feel a bit deprived and disappointed and then you’ll raid the kids’ dairy milk stash because that’s what you wanted in the first place.
So, we suggest you ask the Easter Bunny to bring fewer, better-quality Easter Eggs with some dark chocolate and some of whatever you and your family like. And while Easter is a time for chocolate it’s also a time for family and, for many, for faith. You’ll enjoy your Easter Eggs more if you don’t fixate on them and enjoy a range of Easter foods and Easter activities instead. How about boiling eggs in water with food colouring added for old-fashioned family fun? Or perhaps the Easter Bunny could bring some craft activities for some family craft time.
Whatever you do to celebrate we hope you enjoy it. We look forward to seeing our patients again soon after the few days off to rest and reset. We’re always to here to help with your health goals. Call us on 0439379847 to make an appointment with the osteopaths at Holistic Hands Osteopathy for support in living your healthiest life. Have a great Easter everyone.

Recovering from RSI with Osteopathy
The human body is meant to move. It’s not meant to move like a machine in a factory – repetitively performing one action. And yet office work, modern technology and many manual jobs force us to move in such a way. If we’re unlucky Repetitive Strain Injury (or RSI) can be the result. And it can be debilitatingly painful. So let’s talk about recovering from RSI with osteopathy.
The human body is meant to move. It’s not meant to move like a machine in a factory – repetitively performing one action. And yet office work, modern technology and many manual jobs force us to move in such a way. Even our leisure time is invaded with some sports, hobbies and instruments encouraging limited, unbalanced, repetitive movement patterns. If we’re unlucky Repetitive Strain Injury (or RSI) can be the result. And it can be debilitatingly painful. So let’s talk about recovering from RSI with osteopathy.
What Is RSI?
Repetitive Strain Injury, also called Occupational Overuse Syndrome, is really a descriptive term for overuse injuries rather than a specific diagnosis. The condition can affect any part of the body although it’s more common today in the wrists and forearms due to our reliance on computers and keyboards at work. Carpal Tunnel Syndrome is a type of RSI, as are bursitis and tendonitis. We have a lot of names for it: tennis elbow, texter’s thumb, housemaid’s knee, trigger’s finger, Rubik’s wrist (when Rubik’s cubes had everyone obsessed). The list goes on. In fact, when the condition was first described back in 1700 by Italian physician Bernardino Ramazzini after observing industrial workers, he noted more than 20 categories of RSI. It's simple really - repetitively performing one action without rest can cause inflammation and damage to the body’s soft tissues and nerves. Symptoms can include tingling, numbness, shooting pain and burning sensations, excessive weakness and fatigue, and clumsiness.
What to do about it?
Firstly, please don’t ignore the mild, early symptoms. A small annoyance can become chronic pain if left untreated and continually exacerbated. Now some commonly given advice is to stop doing the activity causing you pain. But as osteopaths we know that’s sometimes not realistic or desirable: a guitarist with a gig coming up can’t just stop practising and a keen tennis player shouldn’t have to give up the sport they love. And we all have to work!
So, what can be done to prevent it?
Ergonomics
Take the time to ensure your work (and play) space is ergonomically sound. Check that your desk, chair and monitor are set at the right height. Similarly, make sure you’re playing with the right sporting equipment for you.
Rest
Take breaks throughout the day and move differently during them. The repetitive nature of typing, playing the piano or swinging a golf club is a problem, but so too is the limited range of motion those actions take you through. Take a moment to stretch and move in an alternative pattern (a few wrist rotations if you’ve been typing for hours for example.)
Posture
Working in a misaligned posture places extra load and aggravation on your body. So sit, stand and move well through whatever activity you’re doing. It’s important to note, that having your environment set-up with ergonomics in mind will help with this, but even the best chair can be slumped in! If you’re really too tired to move well then it’s time for that rest we mentioned earlier.
Treatment
Make an appointment with the osteopaths at Holistic Hands Osteopathy by calling 0439379847 today. The sooner you make an appointment the sooner we can help you. If you have only niggling pain, but it’s becoming persistent, please take action before it becomes debilitating. If you’ve taken steps to improve your workstation, implement rest breaks and moved mindfully, but find things have not improved in forty-eight hours, we advise you make an appointment as soon as convenient. But don’t despair if you have left it too long and are suffering chronically. It might take a little longer, but we can still help. It’s what we do!
After an initial consultation to understand your discomfort and its causes, your treatment will most likely include massage, stretching, and possibly the realignment of some affected joints. Your osteopath will also advise you on exercises and stretches to bring relief. While a cure is unlikely to be instantaneous, your osteopath is uniquely skilled to assist in recovery from RSI. By promoting blood flow to stiff or painful soft tissues and returning the body to a balanced alignment, your osteopathic treatment enables the body’s own healing mechanisms to work efficiently.
We look forward to seeing you at the clinic and helping you back to tennis, golf, gardening, guitar-playing, writing, sewing (or working) with less pain.

Injury blog: Spondylolisthesis
Hello readers! Our blog this month focuses on a spinal condition that in the sports world most commonly affects cricketers and gymnasts, but in reality, can affect anyone! The condition is known as spondylolisthesis (pronounced ‘spon-di-lo-lice-thee-sis’) and most commonly affects the lowest segments of the lower spine region.
Hello readers! Our blog this month focuses on a spinal condition that in the sports world most commonly affects cricketers and gymnasts, but in reality, can affect anyone! The condition is known as spondylolisthesis (pronounced ‘spon-di-lo-lice-thee-sis’) and most commonly affects the lowest segments of the lower spine region.
What is spondylolisthesis?
Spondylolisthesis is the slipping forward of one vertebra on another. This most commonly occurs at the L5 segment (the lowest vertebrae in the lumbar spine), which slips forward on the S1 segment of the sacral bone. The runner up? L4, which is also a commonly affected area.
There are a few different causes of this condition, and so it has been classified into different types. There are five categories of spondylolisthesis. These are:
1. Degenerative: Occurs due to degenerative changes to the spinal facet joints and discs
2. Isthmic: Occurs due to a bone defect in a part of the vertebrae known as the ‘pars interarticularis’
3. Traumatic: Occurs following a trauma that results in a fracture of either the spinal facet joints or pars interarticularis
4. Dysplastic: Occurs due to a developmental defect of the vertebrae which alters the direction of the spinal facet joints, leaving the segment(s) open to slippage in the area where they are partially held in place by the facet joints.
5. Pathologic: Occurs secondary to a medical problem such as infection or cancer
In theory, any process that leads to the weakening of the supportive structures of the spinal segments (i.e. the bones, ligaments, discs, muscles) can lead to abnormal movement of the spine.
Grades of spondylolisthesis
Spondylolisthesis is further classified based on the amount of slippage that has occurred:
• Grade 1: Between 0-25% of the vertebral body has slipped forward on the vertebrae below
• Grade 2: Between 25-50% has slipped forward
• Grade 3: Between 50-75% has slipped forward
• Grade 4: Over 75% of the vertebral body has slipped forward
The most commonly reported grade of this condition is grade one, accounting for approximately 75% of all cases.
Signs and symptoms
These vary depending on the cause, but can include any or all of the following:
• Low back pain, including pain in the buttocks
• Pain along the back of the thigh which rarely goes lower than the knee
• Tight hamstring muscles
• Changes in walking pattern
• Pins and needles and/or numbness down the legs
• Bowel and bladder dysfunction (in more severe cases)
If you come to us with low back and/or leg pain, we are trained to work out exactly what is going on based on your symptoms and medical history. We will ask you lots of questions to begin with to dwindle our list of potential diagnoses to just one or two. Then we’ll get you to move and through a thorough movement assessment, will be able to come to a specific diagnosis that we will work with you to treat.
Sometimes we may require the help of imaging to rule in or out spondylolisthesis, depending on the severity of symptoms and how much it is impacting your life. In these cases, we will send you off for an x-ray which can detect this issue.
Treatment
Most cases of spondylolisthesis can be managed conservatively, meaning non-surgical options are chosen over a surgical one. When this injury occurs, the instability of the particular spinal segment can lead to many of the signs and symptoms mentioned above. One of the main goals of treatment is to increase stability around the affected area and offload the forces that are acting on the injured area.
We will spend time educating you on the mechanics of the spine. If you understand what is happening to your spine, you will know how to protect it, without adding unnecessary stress to the area. We will also advise on appropriate footwear, as well as standing, seated and sleeping postures. Being obese or overweight is also a risk factor for developing, as well as maintaining this problem. If you need to lose weight, we can help you formulate a plan to get there.
Exercise to increase core stability, as well as flexibility of tight muscles is a very important part of therapy as this will reduce the need for external supports such as braces in the long term. And of course, not forgetting our wonderful hands which will get to work on your muscles and joints to reduce tension and tightness, while increasing range of motion.
All of the above treatments will help you to manage pain, increase function and get you back to work or sport or gardening… Whatever your goal is! Call us today on 0439379847 if you have low back pain, or even if you already have a diagnosis of spondylolisthesis, and we can help you formulate a recovery plan to get you on the road to better health.

Fractures Let’s ‘break’ it down
Have you ever broken a bone? We hope you haven't, but it’s a common injury that happens to people every day! Any break in the structure of a bone is known as a ‘fracture’. We’ve written a quick guide to understanding all the lingo relating to fractures below. Let’s check it out!
Have you ever broken a bone? We hope you haven't, but it’s a common injury that happens to people every day! Any break in the structure of a bone is known as a ‘fracture’. We’ve written a quick guide to understanding all the lingo relating to fractures below. Let’s check it out!
Causes
Fractures are usually caused in one of three ways:
• Excessive force: This can be through either a direct force to a body part (i.e. a high tackle in football which breaks the shin-bone) or an indirect force (i.e. having your foot planted and twisting your leg which leads to a fracture of the shin-bone).
• Repetitive stress: These result from repetitive, strenuous activities like running or jumping.
• Other disease: These are fractures secondary to another disease process in the body which leaves the bone more prone to breaking. This may be a hereditary disease like Osteogenesis Imperfecta (aka Brittle bone disease) or as a result of cancer or infection.
Types of fracture: General description
Fractures are broadly classified into two main types:
• Closed: The bone fractures and the overlying skin remains intact.
• Open: The bone fractures and protrudes through the skin exposing the bone and other tissues to the elements. These types of fractures are prone to becoming infected, which complicates everything.
We can also classify fractures on whether they are:
• Complete: A clean break of a bone into two or more pieces
• Incomplete: The bone is not completely broken with some of the outer structure of the bone remaining intact.
Types of fracture: Now let’s REALLY break it down!
Each fracture can also be given a more specific description based on where exactly the bone is broken and in what way it has broken:
• Transverse: A horizontal break across the shaft of a bone.
• Linear / fissure: A vertical break along the shaft of a bone.
• Oblique / spiral: A diagonal, or as the name suggests, spiral type fracture around the shaft of a bone.
• Greenstick: One side of a bone has broken but the other side remains intact. This is common in children where bones are much more flexible than adult bones.
• Comminuted: The bone is broken into more than two pieces, possibly into several fragments
• Impacted: Two parts of a bone fracture are forced into one another
• Crush: Usually seen in the spine caused by vertical and forward bending forces down through the vertebrae
• Hairline: A tiny crack in the bone — these are so small that they are commonly missed on an x-ray!
• Avulsion: A piece of bone is ripped away from the main bone by way of tendon or ligament injury. (Remember tendon attaches muscle to bone and ligament attaches bone to bone).
Which type of fracture have you had in the past? We hope this guide will help you work it out. Next time you come across a fracture (fingers crossed you don’t) you’ll know exactly what the doctors are talking about!
Stay safe!

Injury blog: Winging of the shoulder blades
Hey everyone! We hope you are keeping well. We’re carrying on with life as close to normal as possible, so here is your monthly reading material. Perfect time for a tea or coffee we say! This month we’re taking a close look at the shoulder, specifically a condition that affects the shoulder blade. Do you have, or have you ever seen someone whose shoulder blades stick out on their back and look a little bit like wings? This condition is aptly named ‘winging’ of the shoulder blades. Read on to find out more!
Hey everyone! We hope you are keeping well. We’re carrying on with life as close to normal as possible, so here is your monthly reading material. Perfect time for a tea or coffee we say! This month we’re taking a close look at the shoulder, specifically a condition that affects the shoulder blade. Do you have, or have you ever seen someone whose shoulder blades stick out on their back and look a little bit like wings? This condition is aptly named ‘winging’ of the shoulder blades.
Anatomy
Osteopaths love a bit of anatomy! The shoulder blade or ‘scapula’ is a largely flat bone that sits on the back of the rib cage and is an important ingredient in what makes up the various joints of the shoulder. As well as the larger flat part, a few extra lumps and bumps makes for a very odd shaped bone when looked at in isolation. One of the bony protrusions actually makes up the ‘socket’ part of the ball and socket joint in the shoulder. The ‘ball’ part being made from the head of the upper arm bone (aka the ‘humerus’).
Interesting fact… There are 18 muscle attachments on the shoulder blade. It is through fine balancing of these muscles which keeps the shoulder blade stabilised and flush to the back of rib cage, and allows us to move our shoulders through an extremely large range of motion. As you can imagine, keeping all of these muscles in full working order takes a bit of co-ordination. And with so many players involved, there is room for dysfunction to creep in and movement to become affected. Sometimes the dysfunction is great enough to cause the shoulder blade to flip outwards from the rib cage, and this is what we refer to as ‘winging’.
Causes of winging
The causes of shoulder blade winging can be broadly broken down into:
• Muscular: As we previously mentioned, lots of muscles are responsible for controlling the position and movement of the shoulder blade. Injury to these muscles, or an imbalance in the strength, length and function of the muscles over a prolonged period may lead to this issue. The main muscles involved here are the Serratus Anterior (a muscle which attaches to the ribs and the underside of the shoulder blade), and the Trapezius (a kite shaped muscle which covers the back of the neck, shoulders and upper back… Aka ‘traps’). It’s more complex and there are more muscles involved, but these are the key players when it comes to winging.
• Neurological: Muscles require a nerve supply in order to move, so if any of the nerves that supply the key players (i.e. Serratus and Traps) are injured, this can stop the muscles from being able to perform their job. Nerves can be injured through entrapment, where something presses on a nerve as it travels from the spine down to the muscle it supplies. Other causes may be from acute traumas as seen with car or sporting accidents where the shoulder takes a direct blow while the arm or neck are suddenly pulled.
Other ways these injuries may come about include prolonged wearing of a heavy backpack, complications following surgery, or as a result of a viral infection that affects the nerve.
Signs and Symptoms
The main sign is a shoulder blade that doesn’t sit snug to the rib cage, particularly when trying to move the arm upwards in front of the body or out to the side. Many people with scapula winging feel no pain whatsoever, but this can be a very painful condition if the cause is from a severe nerve injury. Another key sign is the inability of a person to lift their arm above their head.
Treatment
The treatment of shoulder blade winging very much depends on the cause. If the shoulder blades are winging because of a muscular imbalance, these are a little easier and faster to rehab. After careful assessment of your shoulder, neck and other spinal movements, we will aim to restore full functioning of the muscles that control the position and movement of the shoulder blades. This might include techniques which aim to lengthen short or tight muscles which are pulling the shoulder blade out of position. If there is a weakness to a particular muscle or group of muscles, we will also prescribe you strengthening and movement re-training exercises which aim to return the shoulder blade to its functional position.
Winging caused from nerve entrapment or injury is notoriously harder to treat. If entrapment of the nerve is caused by muscular tension in another part of the body, or because you’ve been carrying a heavy backpack for too long, then we will work on the relevant muscles and nerves to release the entrapment and pressure. We might also need to adjust how you wear your backpack and how much weight is inside while we focus on improving your physical impairments. Nerve-related injuries can take much longer to resolve. Winging caused by paralysis of the nerve which supplies the Serratus Anterior muscle has been known to take up to two years to resolve. The good news is, most people will make a full recovery in this time with surgical procedures saved only for more complex or unresolved cases. Which if you ask any Osteo, is always the goal!
If you notice winging of the shoulder blades, or difficulty with achieving full shoulder range of motion, then get in touch today on 0439379847 and get you on the road to recovery as soon as possible.

Bracing: when it is helpful and when it isn’t
A very common question we get asked at Holistic Hands Osteopathy is “Do I need to wear a brace to help with my injury?” Well this is very much a ‘depends’ sort of answer. It depends on the injury, where along the injury process you are and your personal circumstances.
A very common question we get asked at Holistic Hands Osteopathy is “Do I need to wear a brace to help with my injury?” Well this is very much a ‘depends’ sort of answer. It depends on the injury, where along the injury process you are and your personal circumstances.
Let’s first outline the advantages of wearing a brace and give some examples of when you might need to wear one.
Braces are items we place on a body part, usually over and around a joint, to provide extra stability to that area. They come in different forms but are generally quite flexible and elastic to ensure they move with the body, whilst being strong enough to protect the joint simultaneously. Some braces are quite movable whilst others can lock a joint in a particular position.
When is it helpful?
The advantages of bracing include:
• Providing stability to an injured body part to aid with treatment, rehabilitation and return to sport or work scenarios
• Allowing faster healing by limiting movement at an injured body part
• Reducing pain by de-loading injured structures
• Can be easily put on and removed for any given situation
• Are widely available and affordable
A common injury where you may need to use a brace is in the early stages of a moderate to severe medial collateral ligament (MCL) sprain of the knee. Imagine your knee has been forced inward whilst your foot is planted on the ground. If the force is great enough, the ligament stretches, tears and the stability of the knee is compromised. In this case, a brace is helpful to stop the knee from falling inwards again, which would interrupt the healing of the ligament. As healing progresses, the brace can be used less frequently or removed altogether to allow for more movement and activity. Other examples where a brace may be required include:
• Wrist and ankle sprains
• Tennis or golfer’s elbow
• Knee cruciate ligament sprains
• Pelvic instability (these are particularly helpful during pregnancy)
• For stabilisation and re-training of scoliosis cases (i.e. abnormal spinal curves)
When isn’t it helpful?
One of the most common negative effects of bracing that we see is over-reliance. When someone has injured their ankle playing netball, part of the rehab process to get them back on the court quickly may be to wear a brace to provide them with the confidence to play to their full potential without fear of re-injury. This is all well and good as long as they wean off using the brace as rehab progresses. Many people end up wearing the brace as a safety net for 6 months, a year, or even longer because they are scared of re-injury. If you rely on a brace for support, it means the body part that was injured won’t have the necessary forces placed through it to ensure a full recovery to a pre-injury state. This could affect many factors including muscle strength, ligament stability and the body’s ability to know where the joint is in space (a.k.a ‘proprioception’). In order to return to that state, it's necessary to move and exercise completely unaided.
Other disadvantages include:
• Failure to achieve full joint range of motion post-injury
• Possible muscle wasting
• Increased loads placed on other body parts, which can risk another injury elsewhere
Our best advice to you is to never see a brace as a replacement for good movement and rehab. Always follow the advice of your practitioner as to when you should and shouldn’t wear a brace. If you have any doubts or questions, please call us on 0439379847 to discuss.

Osteoarthritis: aging and your body
This month we are turning our focus to the elderly - an ever-growing population. In a clinical setting, us Osteos see our fair share of older patients, and a common degenerative condition affecting the elderly population is osteoarthritis (OA). This most commonly affects the joints in the hips, knees and spine - particularly those of the neck and lower back. Read on to find out what OA is, what you may experience and what to do if you think you have it.
Hello readers and welcome to October’s blog post! This month we are turning our focus to the elderly - an ever-growing population. Did you know that there are approximately 700 million people in the world aged 60 and over? And did you know that it is estimated that by 2050, there will be around 2 billion people on the planet that fall into this age bracket? That’s just over 30 years away! That’s quite difficult to comprehend, but with people beginning to work and live longer, it’s important that the elderly population get the attention and care they need to stay healthy and active; so they can enjoy the quality of life they deserve.
You might think that as people get older, they become less active and therefore are less likely to injure themselves. This may be true to a degree, especially once reaching retirement age, but the elderly population are generally an active population and are just as much at risk of injury as the next person. A 60-year-old person might not play footy or run around the basketball court as much as a teenager might, but they have other things to contend with - an ageing body with years of gradual degenerative change and weakening that we all experience at some point as we go through life. One of the most common causes of injury in the elderly is falling. Unfortunately, as the body ages, it becomes more prone to falls. This usually boils down to a combination of individual factors (i.e. having multiple diseases, poorer eyesight, or general weakening of the body) and environmental factors (e.g. trip hazards around the home setting). Some of the most commonly seen injuries sustained from falls include fractured hips, arms and forearms, cuts and lacerations, as well as head injuries.
In a clinical setting, us Osteos see our fair share of older patients. It’s less likely we’ll see someone in the acute setting immediately following a trauma like a cut, laceration or in many instances where a fracture is suspected, but it does happen. It is much more likely however, that we will see patients experiencing pain related to postural strain (think about the retiree who sits around a lot), or from degenerative changes in the body. A common degenerative condition affecting the elderly population is osteoarthritis (OA). This most commonly affects the joints in the hips, knees and spine - particularly those of the neck and lower back. It’s no coincidence that these are the main weight-bearing joints of the body.
So what is OA?
OA is a condition affecting the synovial joints in the body (the joints between two bones in the body that have a lubricating fluid between them). It is characterised by changes to the cartilage and underlying bone, as well as inflammation and irritation to the soft tissues that help to hold the joints together - known as the synovium - it’s the tissue that forms the lubricating fluid that sits between the joints.
Primary OA refers to changes in the joints that relate to the ageing process. It will often run in the family, so if your granny or dad has it, you may be more at risk to develop it. Secondary OA is arthritic change from any other cause. For example, following on from trauma, repetitive stress, poor posture, or from diseases such as gout.
Signs & symptoms
The main symptoms (things the person experiences) of OA include pain, stiffness, poor joint function and muscle weakness. Signs (things we look for in the clinical setting) that a joint is degenerated include popping and clicking, poor range of motion, bone and joint swelling, deformity and instability.
What to do if you have or think you have OA
First things first, book an appointment to see your local Osteo. After questions and assessment, we’ll get to work on your body and putting you on a pathway to moving better. There is a good chance your arthritic joint is paining you because you aren’t moving well, and the joint is being loaded incorrectly. The good news is, we know how you should be moving, and what needs to be done to get you there. We’ll aim to reduce your pain down by releasing tight and over-worked muscles and mobilising your stiff joints. Mobilising the joints helps to increase range of motion and will help promote production of the lubricating synovial fluid that sits between the joints to allow smooth fluid movement. You should get off the treatment table feeling less pain and moving better. There is a good chance you’ll need to do some form of strengthening to the surrounding weakened muscles, so the joint is more supported when you move it. More good news, we know which exercises will be beneficial to get you on the path to stronger muscles. Unfortunately, we cannot claim to cure your OA, but we can certainly get you moving with less pain or in an ideal situation, no pain at all.
What’s the outlook with OA?
More often than not, if caught early, significant changes can be made to stunt the progression of this degenerative condition. So, don’t ignore pain, it’s your body’s way of telling you something isn’t right. With early treatment, the best possible outcome will be achieved. If you pop into the clinic and we determine your issue is not OA-related, we can provide you with a sense of relief and get you on the right track for your situation (a positive outcome, either way!). In severe cases, you may require the opinion of a specialist orthopaedic surgeon. Sometimes people require joint replacements and can go on to live a very good quality of life with a new hip or knee for example. Always see your Osteo first though. Using our skills, we can possibly keep you from having to go under the knife a bit longer, and maybe even at all. Worth a shot don’t you think?!
Lumbar disc prolapse: Symptoms and treatment
A possible and relatively common cause for searing back pain is a lumbar disc prolapse. Sit back with a coffee and let us take you through the ins and outs.
It’s moving day and you’ve been running around packing, unpacking, lifting boxes and awkward furniture all day. You can’t stop though because there’s still more to do. It’s onwards and upwards with another load in the back of the Ute. You bend down to pick up the umpteenth box of the day and bang and you’re hit with excruciating low back pain and a shooting pain down the back of your leg. It’s crippling and you’re struggling to catch your breath and stand up straight. It’s a scenario unfortunately a lot of us are familiar with, but what has caused this searing pain? One possible and relatively common cause for such pain is a lumbar disc prolapse. Sit back with a coffee and let us take you through the ins and outs.
What is a disc and what just happened when I bent down?
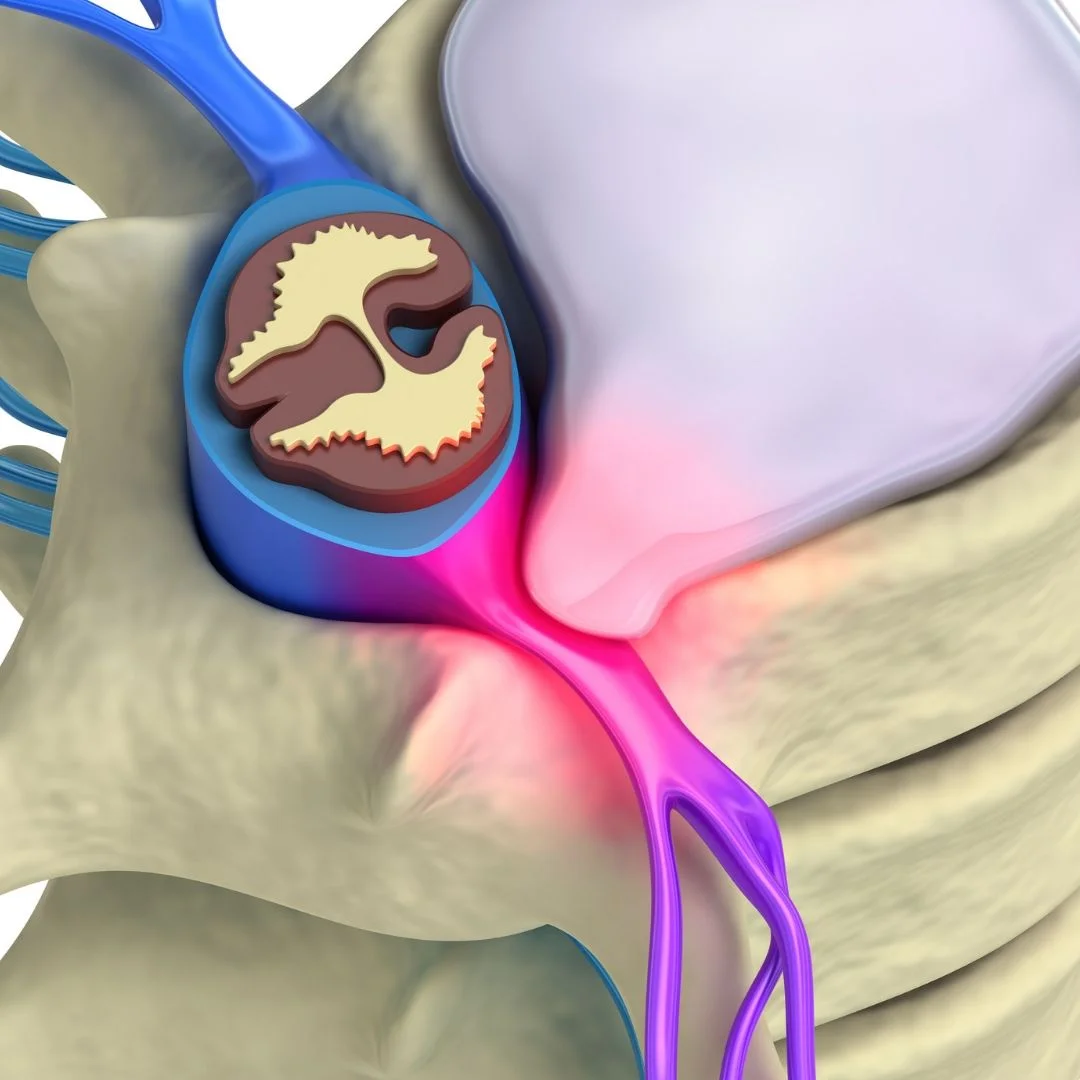
Your spine is made up of many vertebrae spanning from the neck all the way down to the tailbone. Between each vertebra sits an elastic-like structure called a disc. The disc is made up of a tough outer section called the 'annulus fibrosus’, and a gel-like inner section called the ‘nucleus pulposus’. The discs work to separate the vertebrae to allow movement, as well as provide shock absorption to forces acting on the spine during movement.
Common causes of disc prolapse include trauma and degeneration of the disc tissue as a result of poor posture (for example lots of slouching or slumping) and repetitive bending movements. When we bend forward, particularly when we bend forward under load (like with our house mover above who had been repetitively picking up and putting down heavy boxes), the forces acting on the discs, and especially the inner nucleus, increase drastically. Over time these repetitive movements may cause small micro-tears in the layers of the outer annulus, which weakens the overall structure of the disc. Slowly, the nucleus gets forced out and a small bulge may occur (there is often no pain at all at this stage). If these movements continue, or if you go to pick up that box which is just too heavy for you, the force is too much and the bulge can progress into a larger protrusion. Like with any injury, the initial response of the body is inflammation. The presence of inflammatory chemicals alone can cause irritation to the surrounding nerve tissue as it exits the spine, or you may get actual contact of the disc on to the nerve itself, causing impingement. This is when you feel pain and know that all is not well.
What should I expect to feel when this happens?
The signs and symptoms of a disc prolapse can vary greatly depending on the type and severity of the prolapse, and where the spine is affected. A prolapse may happen slightly out to one side of the disc affecting only the nerves on that side of the body (this is most common). Or it may occur in a backwards direction, potentially affecting nerves on both sides of the body. A small bulge may only yield mild symptoms, whereas a large prolapse may cause more severe symptoms. Interestingly, this is not always the case though.
Some of the symptoms you may experience include:
• Low back pain
• Pain running down the front, side or back of the leg
• Pins and needles or tingling down the leg
• Numbness down the leg
• Muscle weakness (this may manifest as losing the ability to lift your foot)
The most common disc prolapse affects the L5/S1 disc (the lowest disc in the spine) and will give symptoms down the side and back of the leg. Your practitioner will ask you lots of questions and do lots of tests to determine exactly what area is being affected.
How do we treat disc prolapses?
Initially you may be in a lot of pain and simple movements may be very difficult to perform, like standing up straight, for example. This is because the body is trying to protect you from doing further damage. Once inflammation occurs, the body needs a few days to deal with what has happened. So, if you come to see your Osteo straight away, don’t expect to feel better after one visit. In fact, it is quite possible you will feel worse in the coming days before you start to feel better. The advantage of seeing your Osteo early on is that they can educate you on the do’s and don’ts, tell you what to look out for and inform you what to expect going forward. Often the unknown is scary, but your Osteo will be able to ease your mind, even if not the pain immediately. Us Osteos like inflammation. It’s the body’s way of protecting the injury and getting organised for repair. So, although it may be painful, it is good to see it through without intervening too much.
Early on, we’ll get you moving better. We will also give you breathing, relaxation and core activation exercises to help the body better cope with the pain. A disc will often prolapse because of poor core stability, so getting you on the path to rehabilitating your core is good early on. When it is possible, we will relax the tight muscles and reinstate movement to joints that may have seized up and become restricted following the injury. Our focus is to ensure the fluids of the body (i.e. blood, joint fluid, and lymphatic fluid) are moving freely around the body. When injury occurs, these fluids can become congested and a bit stuck around the area, and sometimes need a little help to get moving again. This will ensure a speedier recovery. The injury site will need lots of fresh blood to the area, while the lymphatic system will need to be flushed – ridding the area of all the bad stuff. Depending on the severity, discs generally take around 3-6 months to fully recover.
Your Osteo is trained to help you through the injury process, so you can rest assured you are in safe hands. We know when and how to treat and know what to look for to ensure you are seen by the right people if it’s required (this might include your GP or a specialist if necessary). If you think you have a disc prolapse or have previously been diagnosed with one and need help managing it, then look no further. Call us today to book your appointment.

Introducing chronic pain and how to treat it
Hello everyone, and welcome to our July blog! This month we are going to be talking about pain.It’s a complex topic, so we have devised a little introduction to break it down so you can understand more on chronic pain - all in the name of National Pain Week which is due to take place at the end of this month.
Hello everyone, and welcome to our July blog! This month we are going to be talking about pain. We can’t believe it’s already halfway through the year. Time certainly does fly! But for the 3.24 million Australians living with chronic pain, it’s just more time spent battling the daily hurdles - getting out of bed, working, socialising, being a parent, everything really! Being in pain for a long time can be debilitating and have a huge impact on a person’s life.
Taking into account running healthcare costs, time and money lost at work, as well as decreased quality of life, the total cost of chronic pain in Australia in 2018 totaled $139.3 billion! It’s a growing problem with a prediction that over 5 million Australians will be affected by chronic pain by the year 2050. As Osteopaths, we work with and treat people who experience chronic pain day in and day out. It’s a complex topic, so we have devised a little introduction to break it down so you can understand more on chronic pain - all in the name of National Pain Week which is due to take place at the end of this month.
What exactly is pain?
Pain is an unpleasant experience. Ask 100 random people in the street if they like to experience pain, and there is a good chance 100% of those people will say “no”. However as unpleasant as it is, pain is an essential part of life. It is our protection mechanism. When we injure ourselves, we feel pain. Sometimes before we even get to the injury stage, we can feel pain… Pain will also stick around for a bit following an injury to remind us that healing needs to take place and that we need to protect the injured area from further damage. It’s a sophisticated alarm system and you have your brain to thank for all of this. Pretty cool huh?
Interestingly, there are people on this earth who cannot and have never felt any pain at all. These people may have a very rare condition called Congenital Insensitivity to Pain (CIP). They are basically born with the inability to feel pain. You might think this could be pretty beneficial - going your whole life without pain. How awesome would that be?! In reality, this is a very serious condition, and many who are born with it have a drastically shortened life. Mainly because injuries and illnesses can go unnoticed, potentially putting their life in danger. For example, cuts and burns will go missed, because they lack the important alarm system we were talking about above. Pain is a lifesaver.
Acute vs chronic pain
Pain can be very simply divided into two types, acute and chronic. Acute pain is the pain felt when we fall or cut ourselves, strain a muscle or sprain a ligament. When injury occurs, special sensors in the vicinity of the injury detect that something is wrong, send a message along nerves to the spinal cord and up into the brain. Your brain will process this information (very quickly) and will send a message back as a pain signal. You say “ouch”. Over the coming days and weeks, the injury heals and the pain disappears. During this process, your brain will have formed a memory of the event, and this helps you to steer clear of similar dangerous situations in the future. Protection at its best! For purposes of time, acute pain is pain that is felt for any time up to six weeks. Sub-acute pain (a sub-set of acute pain) is pain felt anywhere between six weeks and three months.
Chronic pain
Chronic pain, also known as persistent pain, is essentially pain that has lasted longer than three months and is a very different kettle of fish to acute pain. In many instances, it is pain that is felt way beyond tissue healing times and is extremely complex in nature due to the involvement of different body systems. And, most importantly, the persons belief about what pain is. The initial cause may be from a fall or car accident, just like with any acute injury. It may also be caused by diseases such as arthritis, cancer or migraines (as well as many others).
Why chronic pain develops is a complicated process. In a nutshell, generally tissues have healed, yet the brain is still perceiving a threat. This is due to changes in the nerves carrying signals to the spinal cord (the peripheral nerves) and changes in the spinal cord itself. Essentially, these nerve tissues become highly sensitised and end up sending faulty or misleading information to the brain. The brain perceives this information as still threatening, and the result is ongoing pain. It is much more complicated than that, but this gives you the gist of what is going on.
It is important to understand that when someone is in pain for long periods of time, they can start to become affected in other ways. Depression and anxiety regarding pain is commonplace. A person’s beliefs about pain will also begin to affect their behaviour. For example, they will start to avoid certain movements due to fear of injuring themselves further (which can cause other musculoskeletal issues). In psychological terms, this is known as exhibiting fear avoidance behaviours.
Treating chronic pain
The longer the cycle of chronic pain persists, the harder it is to treat. Unfortunately, treatment is not as simple as applying first aid principles like rest, ice and compression, followed by massage, mobilisation and rehabilitative exercise programs. It is still important to treat the person’s movement dysfunctions of course, but treating the depression and anxiety whilst educating the person on what is actually happening is just as important, if not more so. Until all facets of a person’s pain experience are dealt with in some way, it is unlikely the cycle will be broken. Therefore, treating chronic pain rarely comes down to just one profession. It requires what we call a multi-disciplinary approach to treatment. So yes, an Osteopath may well be part of the team, but it is likely a person will also require the services of a Psychologist and their GP too. It may be that pain medication will need to be prescribed (although the debate is still out on how effective strong pain medications are in the instances of chronic pain).
Your Osteopath will help to treat you by ensuring your body is moving in the best way possible, and that your tissues are at their optimum health. They may also advise you on how to improve your sleep patterns and diet, to ensure your body is getting the rest and nourishment it requires. They will advise you on the forms of exercise which may be beneficial and may even be able to give advice on relaxation and breathing techniques. Most importantly, they will spend time with you, educating you on what exactly is going on with your body so that you can begin to understand it yourself— and begin breaking the cycle of chronic pain. It will be a team effort, and they will be with you every step of the way!
We hope you found this blog interesting and educational. If you would like to know more about National Pain Week and further information on chronic pain, please visit http://www.nationalpainweek.org.au.

Carpal Tunnel: Symptoms and treatment
Do you experience tingling into the hand and wrist pain in the night and also during the day when at work? You may be experiencing symptoms of Carpal Tunnel Syndrome. Read on to find out all about about it!
It’s been a long day at the office, the kids are fed, bathed, and down for the night, and it’s time for my head to hit the pillow. Exhausted doesn’t cut it, but I still cannot sleep… What IS this tingling in my fingers and wrist pain I keep getting?! I felt it a bit at work earlier too, but why now? I’m nowhere near a desk or computer!
Sound familiar? Wrist pain is quite common, and one of the most common causes for pain over the palm side of the wrist and hand is Carpal Tunnel Syndrome (CTS). CTS presents when one of the larger nerves that travels from your shoulder down to the tip of your fingers (it’s called the Median nerve) gets compressed as it passes through the wrist. The ‘tunnel’ is a small space in the wrist, made up on one side by the wrist bones (the ‘carpals’), and a soft tissue covering on the other side. Alongside the nerve travels a group of tendons from the forearm, and once all of that has passed through the tunnel, there isn’t a lot of room for anything else. Throw in a heap of repetitive wrist movements over a prolonged period (for example typing at a desk day in, day out), and the structures running through the tunnel can become irritated and inflamed making an already small space even smaller. Once the nerve becomes compressed, symptoms start to creep in.
Signs and symptoms
CTS can be characterised by the following signs and symptoms:
• Burning wrist pain (on the palm side of the wrist)
• Numbness, pins & needles or tingling of the thumb, index, middle and inside part of the ring finger
• Night time symptoms
• Pain that radiates to the forearm, elbow or even the shoulder
• Reproduction of symptoms when compressing or tapping over the palm side of the wrist
As well as repetitive motions of the wrist (seen commonly in desk-based workers, sports people, and even our very own manual therapists), CTS can be caused by some underlying conditions, such as Diabetes Mellitus, Thyroid disease, Rheumatoid Arthritis, high blood pressure, and from fluid retention associated with pregnancy or menopause. Trauma or fractures in the wrist may also lead to this condition. Unfortunately, if you are female, you are also three times more likely to experience this problem.
Treatment
If caught early, this problem can be managed conservatively with a combination of the following treatments:
• Soft tissue release, joint mobilisation/manipulation (contact your local Osteo
• Anti-inflammatory medication
• Splinting of the wrist (particularly at night time)
More severe and persistent cases may require more invasive treatments including having a steroid injection, or possibly surgery to decompress the nerve.
If you have wrist pain, and you think it could be CTS, then our best advice is to visit your local Osteo where you can be assessed thoroughly, diagnosed accurately, and given the best advice and tools to manage your problem. We’ll get you waving goodbye (pain-free) to pain in no time!

Is it Time to Make a Move to the Dark Side?
THE BENEFITS OF CHOCOLATE
We’ve all heard that chocolate has health benefits. That is true, but it depends on which chocolate. Given it’s Easter month, we thought we’d take the opportunity to justify our chocolate love! Read on to find out more.
The Benefits of Chocolate
We’ve all heard that chocolate has health benefits. That is true, but it depends on which chocolate. Unfortunately for you milk and white chocolate lovers (is white chocolate even chocolate?), this article focuses on the dark side of your cravings! Given it’s Easter month, we thought we’d take the opportunity to justify our chocolate love! Here’s our top three health benefits of dark chocolate:
1. High in antioxidants: A good quality dark chocolate with a high cocoa content is packed with useful antioxidants, which helps the body fight the nasty stuff. Our little helpers include polyphenols and flavanols, as well as others. These guys are responsible for helping rid the body of damaging free radicals (small molecules that whizz around the body causing damage to your insides), as well as having many other benefits.
2. High nutrient content: Dark chocolate is not just antioxidant rich, it’s full of other good stuff too. It’s a great source of fibre, iron, magnesium, zinc and selenium, and the list goes on! It also contains some good fats. It’s important to eat in moderation though because although there are many benefits, you will also be consuming a decent amount of sugar and calories (although nothing compared to its milk and white counterparts!).
3. It’s good for the skin, heart and brain: All the above-mentioned benefits can go a long way to improving the health of your skin, heart and brain. The antioxidants present in dark chocolate may help to protect against sun damage, lower levels of bad cholesterol (the ‘LDL’s’ of the body) and improve blood flow to the brain to aid with cognitive function. Win, win, win!
So, are you ready to come over to the dark side now? We think it will be the best chocolate related decision you’ll ever make!